
According to Harvard University School of Public Health, 33% of adults in the U.S. are overweight and 36% are ob⁶ese. Although percentages vary, several sources claim two thirds of American adults are overweight or obese.
With these numbers, one might expect a certain amount of heft to be perceived as acceptable, perhaps even desirable. But not so. Instead, in the United States, labels like fupa, lard, chunker, fatso, and jelly belly are slapped on. And how is this for humor? A collective noun for a group of overweight/obese people: A blubber of fat lads.
Even people who are trying to be polite or helpful say things that sting:

- It’s easy to lose weight …
- You have such a pretty face …
- You’d be so pretty if you lost weight …
- I don’t see you as fat …
- You look great! …
- I’m so fat (when the speaker isn’t) …
- It’s not like you’re obese …
- That (food) looks healthy …
- I’ve always wanted a bum like yours! …
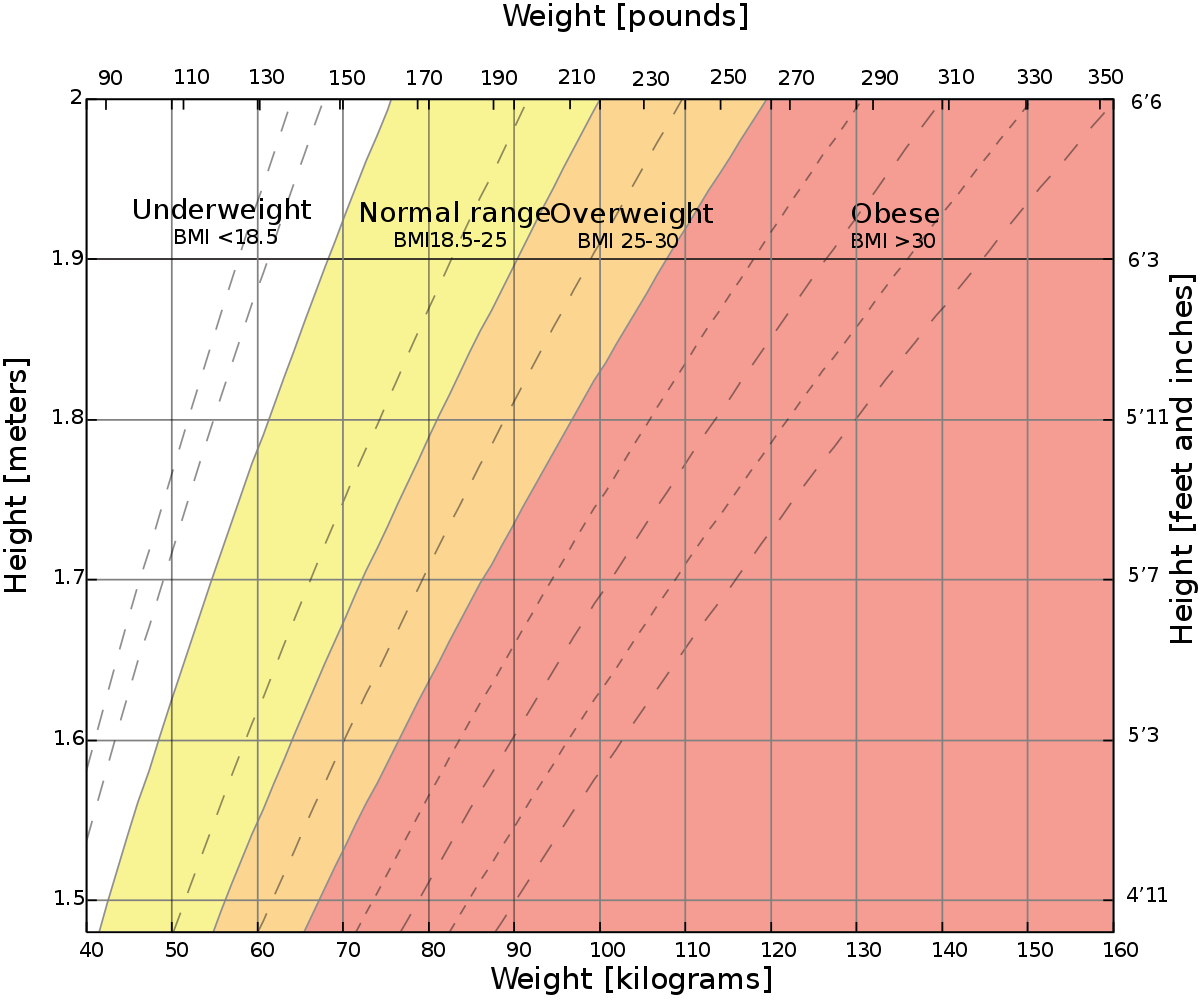
Where Did the Body Mass Index Come From?
Lambert Adolphe Jacques Quetelet, a Belgian mathemetician, developed Quetelet’s Index (later called the Body Mass Index or BMI) in the 1842 as a method of determining the average measurements of French and Scottish men. Quetelet prized homogeneity and thought that the ideal person should be as close to the center of the statistical bell curve as possible. At the time of its creation, Quetelet was very clear that “Quetelet’s Index” was useful solely as a means of predicting the average body size of a population, not to measure or predict anything for an individual, including health.
In 1867, Mutual Life Insurance of New York started using an adaptation of Quetelet’s BMI tables to determine how much to charge policy holders. Within a few years, every insurance company in the market was using different BMI tables with wildly varying numbers to define “healthy” weights, which they then used to set prices for clients.
Even when Ancel Keyes adapted Quetelet’s original findings as a way for doctors to use during medical consultations, he admitted that the BMI was only accurate as measure of obesity about half the time. He also included data only from men, almost entirely white men from relatively wealthy countries.
These early limitations of the BMI calculator continue to cause serious challenges for those trying to use it as a diagnostic tool. Women’s bodies store fat differently than men’s bodies. The cut-offs for defining someone as overweight or obese vary widely among ethnic groups. Scientists created the BMI for children by simply extending downward the existing trend lines for small adults, which makes the data for children particularly unreliable. Older adults have different metabolic needs and may benefit from having a higher BMI altogether.
In 1995, the World Health Organization change the definitions of overweight and obese according to BMI. The American National Insitute of Health (NIH) adopted those standards in 1998; overnight, millions of people became overweight or obese without gaining a pound. This marked the start of the “obesity epidemic” and the “war on obesity” (which has not really had any effect on actual health.)
Obesity Today

Today, the NIH classifies about 1 in 11 adults (9.2%) as having severe obesity.
As a rule of thumb, you are likely morbidly obese if you are more than 100 lbs. over your ideal body weight or have a BMI of over 40.
Women had a higher prevalence of severe obesity (11.5%) than men (6.9%). The prevalence was highest among adults aged 40–59 (11.5%), followed by adults aged 20–39 (9.1%), and adults aged 60 and over (5.8%).
Other obesity data reflect much of the data on other health issues.
Recent national data show that 54.8 percent of Black women and 50.6 percent of Hispanic women are obese compared to 38.0 percent of White women. Rates of obesity are also higher for Hispanic men, in the South and Midwest, in nonmetropolitan counties, and tend to increase with age. However, as discussed above, inherent problems in calculating BMI may misrepresent actual health of people in these populations.
Who Is Fat? Who Is Obese?
Kimberly Truesdale and June Stevens found that perception of one’s own weight may be skewed. Surprisingly, to me, only 22.2% of obese women and 6.7% of obese men correctly classified themselves as obese.
How can this be? Fat people have all kinds of euphemisms for fat. (Curvy, plump, voluptuous, plus-size, zaftig, heavyset, Rubenesque, queen-size, large, thick, plush, stout, hefty, buxom, portly, ample-bodied, curvaceous, puffy, fluffy, etc.)
In the Media
As I reported in an earlier blog (September, 2020) Greenberg et al. reported on their findings of television actors’ BMI after analyzing 5 episodes of the top 10 prime time shows.

- In comparing television actors’ BMI to that of the American public, they found that only 25 percent of men on television were overweight or obese, compared to almost 60 percent of American men.
- Almost 90 percent of women on TV were at or below normal weight, compared to less than 50 percent of American women.
Popular television shows that include people who are obese portray them as comedic, lonely, or freaks. Rarely if ever are they romantic leads, successful lawyers or doctors, or action stars.
In addition, shows like The Biggest Loser promote the perception that obesity is caused by individual failure rather than a mixture of individual, environmental, and genetic sources.
Weight and Mental Health

Defensive self-labeling aside, the results of fat shaming are apparent in many correlates of mental health. Societal stigmas and biases mean that carrying extra weight is hard on one’s mental health.
Late-onset or chronic overweight/obesity predicted low general, social, and academic/school-related self-esteem.
Socially competent people using better strategies for solving interpersonal problems are more readily accepted by peers and valued by adults. Obese individuals, especially teenagers, have deficits in several social skills, which lead to damage to relationships, lower self-esteem and devaluation by social agents.
Children with lower social skills are also at a greater risk of becoming overweight or obese.
Many individuals who are obese also struggle with issues related to their mood, self-esteem, quality of life, and body image. This emotional distress likely plays a role in treatment seeking but also can impact successful treatment.
Weight Stigma
“Anti-fat bias kind of turns up the volume on existing systems of oppression,” says Aubrey Gordon, author of You Just Need to Lose Weight” and 19 Other Myths About Fat People.

Obesity is associated with a higher risk of having certain mental health disorders, including anxiety, depression, bipolar disorder, and eating disorders. Often, this relationship is due to the effects of weight discrimination.
People with a weight problem are more likely to feel alone and describe themselves as lonely. They may feel they might not ever meet the ‘right person’, feel uncomfortable with intimacy, feel they are being judged for their weight, and just want to hide sometimes.
Obesity contributes to negative mental health and poor psychological well-being. Society also highly stigmatizes obesity, which negatively affects social and relational health, as well as inhibiting communication about the topic.
Medical professionals are often guilty of fat-shaming. Patients seeking treatment for problems that have nothing to do with size are instead lectured about why they need to lose weight. As Aubrey Gordon says, “It is one of the great fears of my life, that I will die of a totally treatable or preventable thing because my doctor can’t conceive of me having any other health problem than just being a fat person. That is a fear that follows me every time I go into a doctor’s office.”

The vast majority of people who are overweight or obese according to BMI also have some form of eating disorder, according to Dr. Erin Harrop at Denver University. However, because these patients don’t fit the common perception of looking dangerously thin, the medical establishment classifies thesm as having “atypical anorexia.” This distinction makes it much more difficult to receive an accurate diagnosis. Not only are doctors more reluctant to treat overweight patients with disordered eating, insurance companies are reluctant to cover those treatments.
The social and emotional effects of obesity include discrimination, lower wages, lower quality of life and a likely susceptibility to depression.
To be clear, the mental health issues that are correlated with being overweight or obese are caused by our fat-shaming culture. In societies where people value weight, these stigmas are not prevalent.
Does Personality Cause Obesity?
Who are these overweight and obese people?
In analyses of separate personality traits, openness and conscientiousness were significantly associated with obesity in men, and only agreeableness was associated with obesity in women.

Introverts are more likely to be at a healthy weight. They have lower rates of obesity. In one study of nearly 2,000 people over a span of 50 years, extroverts were heavier than introverts, with more body fat, larger waists, and bigger hips.
The BIH has found positive associations between obesity and the personality traits neuroticism (OR: 1.02) and extraversion (OR: 1.01), and negative associations between obesity and openness to experience (OR: 0.97) and agreeableness (OR: 0.98). (Recall, a positive association means as one goes up, so does the other; a negative association means as one goes up, the other goes down.)

Although there is no single personality type characteristic of the morbidly obese, they differ from the general population as their self-esteem and impulse control is lower. They have passive dependent and passive aggressive personality traits, as well as a trend for somatization and problem denial.
Over-eating may be the result of self-sabotage. A person gets into a cycle of low self-worth and shame, using food to soothe. Obesity can also be seen as a way of showing the world ‘I am worth nothing, stay away, because I am bad.’
Researchers have found four characteristics that typify the ”overweight personality.” You may have low self-esteem, poor self-control (or even eat compulsively), experience mood swings, or be prone to depression and anxiety.
Physical Causes of Obesity
Genes contribute to the causes of obesity in many ways, by affecting appetite, satiety (the sense of fullness), metabolism, food cravings, body-fat distribution, and the tendency to use eating as a way to cope with stress. Some researchers believe they may have identified “missing” genes that potentially contribute to obesity.
It’s important to remember that obesity is a disease, and we shouldn’t blame individuals for it because the causes are not always something they can control. In other words, it’s not your fault if you are obese.
Obese and Healthy
Obesity is definitely a physical health hazard, but poor health is not necessarily inevitable. In a database at McGill University, about 15% or slightly over half a million people were categorized as being obese and metabolically healthy.
If a person is 300 pounds and does not have any other diseases or health complications, then that person is considered healthy. However, the chances of staying healthy with 300 pounds weight are low. Around 99% of individuals weighing this much suffer from several other health complications.
“There is a lot of data that says that fat people generally and fat women in particular postpone care because they know that they are going to be overtly, directly judged by their health care providers and they know that they will get substandard care because of that judgement.”
Essentially, people with obesity can still be healthy. However, what a McGill University study, and prior research, shows is that obesity even on its own carries a certain cardiovascular risk even in metabolically healthy individuals.
Some People Do Manage to Lose Weight
The annual probability of achieving normal body weight was 1 in 210 for men and 1 in 124 for women with simple obesity. The probability declined with increasing BMI category. In patients with morbid obesity, the annual probability of achieving normal weight was 1 in 1290 for men and 1 in 677 for women.
Good news! Children who successfully reduced weight may have equal levels of self-esteem or even better social self-esteem than those being always underweight/normal weight.
The disease of obesity, no matter what it means for your physical body, is not your whole self or your whole life. Obesity does not define you as a person.
Bottom Line: For many people, too much weight is a fact of life. Be aware of the possible (probable) effects of fat shaming on your mental wellbeing!