Everybody has one. But how much do you really know about it?
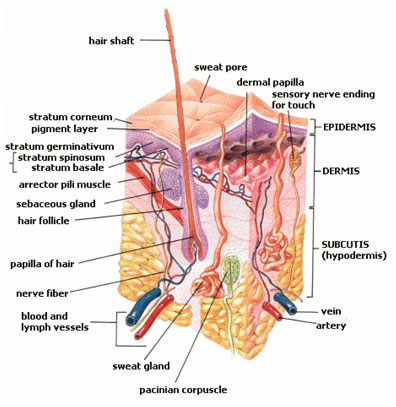
Skin
Let’s start with your largest and most visible organ: skin. When it comes to skin, we tend to notice attractiveness, color, roughness, and wrinkles. But skin is functional as well as ornamental. It keeps everything on the inside from coming out. In addition, it also helps keep us at the right temperature, helps us with touch and sensation, allows us to move without restriction (not too tight or too loose), heals and regenerates constantly, and much more.
You probably aren’t average, but these “average” data will give you an idea of how you compare.
Skin by the Numbers
If you are average, your skin weighs 6-9 or 7.5-22 pounds, depending on your source. According to the NIH Library of Medicine, skin makes up approximately 1/7 of your body weight.
Again, if you are average, you have approximately 21 square feet of skin.
Organ donation can include skin.
The average person has about 300 million skin cells. One square inch of skin has about 19 million cells.
Every second, you produce 25 million cells.
The entire surface of your skin is replaced every month, which put another way means you have about 1,000 different skins in your life! This skin renewal every 27-28 days involves sloughing off the old.
Your skin constantly sheds dead cells, about 30,000 to 40,000 cells every minute! (That’s nearly 9 lbs. per year. On the low end, other sources say you slough off roughly 1.5 pounds of dead skin a year, equal to about 3 ½ cups of sugar.)
Dead skin comprises about a billion tons of dust in the earth’s atmosphere. Indoors, the oil on dead skin cells helps to remove ozone, leaving the air cleaner!
Some sources estimate that more than half of household dust is actually dead skin, others say 70%, but much depends on number of people, pets, etc.
Passengers
Your skin is home to more than 1,000 species of bacteria.
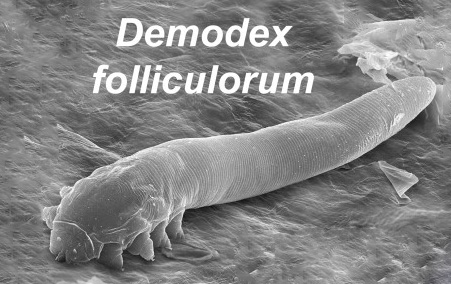
Your face is host to bugs (demodex folliculorum) too tiny to see. Hairlines, eye sockets, and lashes are favorite hiding places. If they get out of control, they can cause skin problems or eye infections.
About 2,400 germs call the belly button home. The average person has 67 different species of bacteria in their belly button.
Weird Skin

Scar tissue is different from normal skin because it lacks hair and sweat glands.
Some of the nerves in your skin are connected to muscles instead of the brain, sending signals (through the spinal cord) to react more quickly to heat, pain, etc.
The color of human skin is determined by the level of pigment melanin that the body produces. Those with small amounts of melanin have light skin while those with large amounts have dark skin.
Genital skin is darker than other skin: nipples, anus, and genitals are more sensitive to sex hormones acting on melanocytes. The contrast increases during puberty and pregnancy.
Your skin has at least five different types of receptors that respond to pain and touch.
Blood and Heart
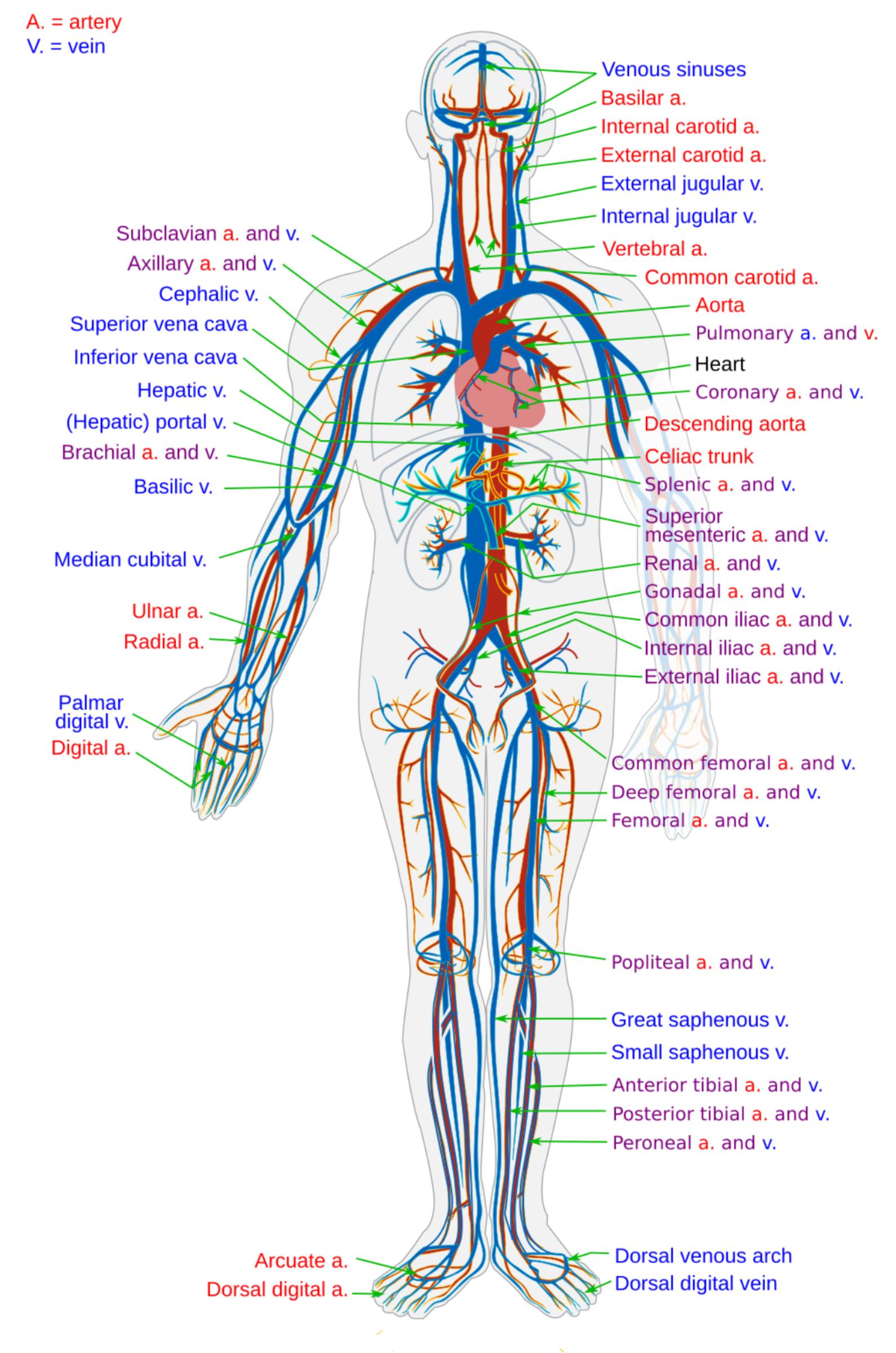
Your skin contains more than 11 miles of blood vessels.
Your blood makes up about eight percent of your body weight.
Laid end to end, an adult’s blood vessels are between 9,000 and 19,000 kilometers long! This includes veins, arteries, and communicating little capillaries that move between both.
Pus is a build-up of white blood cells.
Humans are the only species known to blush.
Your heart beats around 100000 times a day, 36500000 times a year and over a billion times if you live beyond 30.
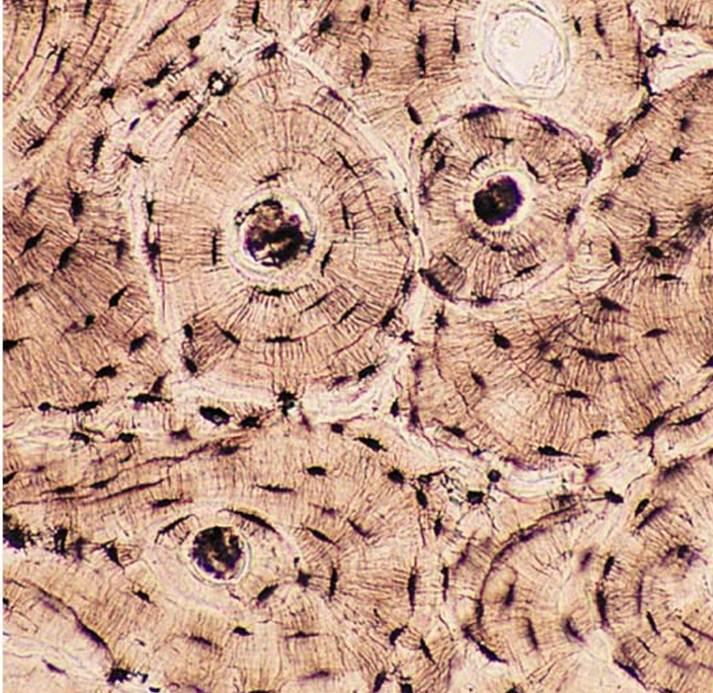
Inside your bones are tiny tubes filled with blood vessels called osteons. They are to bones what rings are to trees. The percentage of large osteons increases with age.
Your eyes blink around 20 times a minute. That’s over ten million times a year!
Sweat
The body has 2.5 million sweat pores.
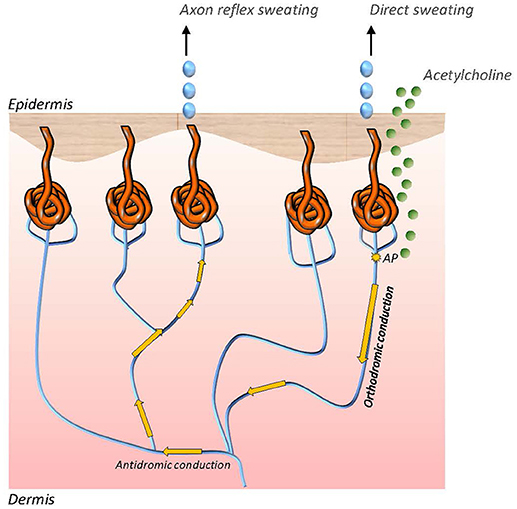
A single square inch of skin has up to 300 sweat glands.
When you’re too hot—or you lose your cool—your nerves send signals to open millions of glands, allowing sweat to flow. It pools by your armpits, palms, feet, head, and private parts.
Earwax is actually a type of sweat! A recessive gene can cause earwax to be dry and flaky rather than viscous and sticky.
Germs love to swim, so they thrive in sweat. Sweat on its own doesn’t smell bad. It’s the bacteria that mix with it.
Body Products
Your mouth produces about one-two liters of saliva each day!
You produce about 40,000 liters of spit in your lifetime. Or to put it another way, enough spit to fill around five hundred bathtubs.

Babies don’t shed tears until they’re at least one month old.
What we eat directly affects urine and feces. For example, you might notice red or pink after bingeing on beets. Or changes in your urine after eating asparagus.
(Note: although asparagus affects the chemistry of everyone’s urine, some people are able to smell it and others aren’t—whether their own or someone else’s.)
We urinate enough every month to fill a bath!
The average nose produces about a cupful of nasal mucus every day.
On average, you fart enough in one day to fill a party balloon.
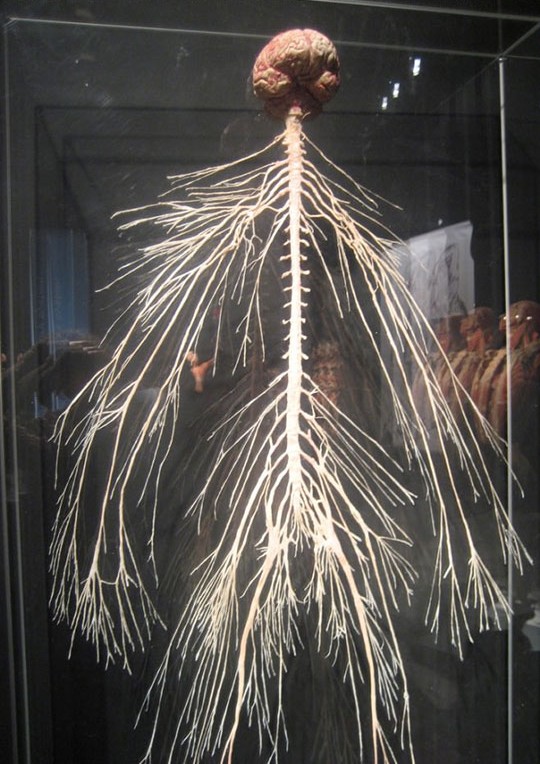
Brain and Nervous System
Your brain is the fattiest organ in the body, approximately 60% by dry weight. It needs essential fatty acids to perform adequately.
The brain uses over a quarter of the oxygen used by the human body.
Your brain is sometimes more active when you’re asleep than when you’re awake. Humans have a stage of sleep that features rapid eye movement (REM). REM sleep makes up around 25% of total sleep time and is often when you have your most vivid dreams.
Information zooms along nerves at about 400k mph!
Everyone is familiar with forgetting, but additionally, our brain re-writes memories each time we think of them, slowly altering or twisting them over time.
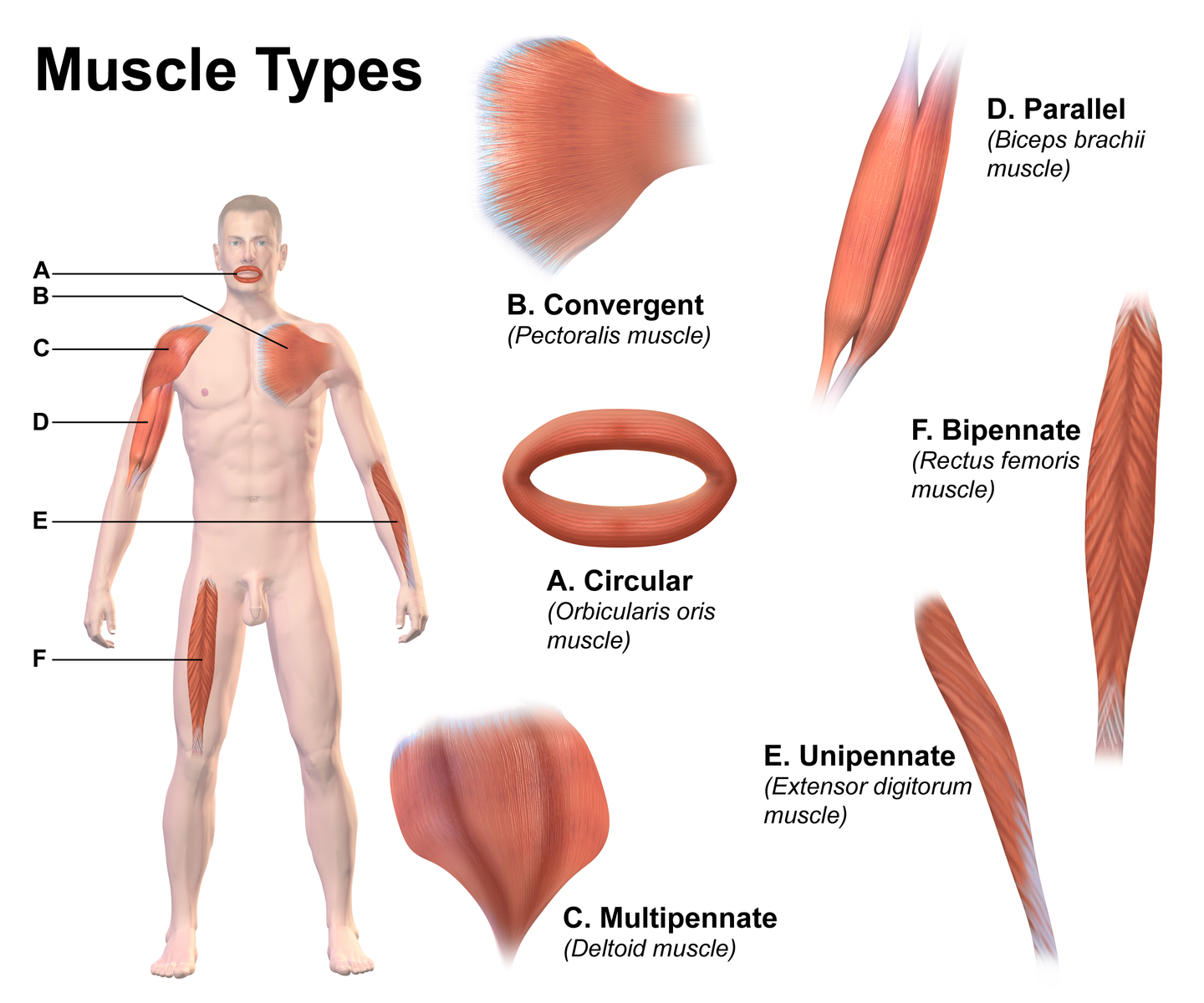
Muscles
The word “muscle” comes from Latin term meaning “little mouse“, which is what Ancient Romans thought flexed bicep muscles resembled.
Your heart is the only muscle that doesn’t get tired.
Gluteus maximus is the Latin name for the largest muscle in your body, your behind. You have two of them, one for each cheek. These powerful muscles serve as a cushion when you sit down, but when flexed tight, they keep you upright.
Few muscles are as hard-working as the tongue. By day, it twists to form the sounds you speak and pushes around the food you eat. While you sleep, your tongue moves saliva down your throat.
The strongest muscle in the human body is the jaw (masseter). A healthy jaw can close teeth with a force of up to 200 pounds, according to the Library of Congress.
Eyes
Your eyes can get sunburned. The symptoms include headache, eye pain and redness, tearing, blurred vision, twitching, and feeling gritty. Sunglasses can prevent sunburn, and symptoms typically resolve themselves after 48 hours.
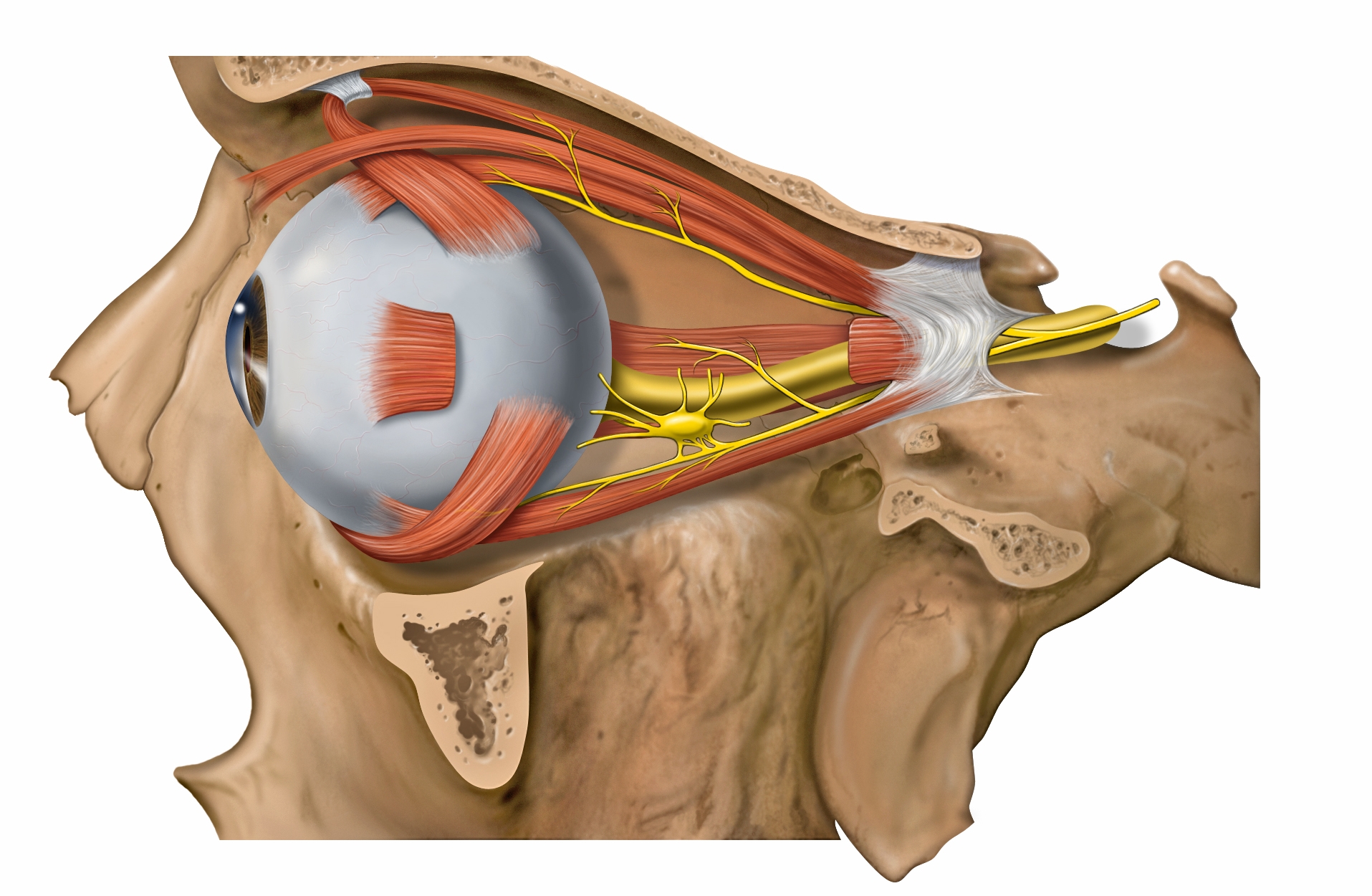
Your eye is your fastest muscle. The orbicularis oculi is capable of contracting in less than 1/100th of a second.
A blink typically can last 100-150 milliseconds.
Infants blink only once or twice a minute while adults average around 10.
Women blink 19 times per minute compared to 11 per minute for men. This may relate to estrogen levels, which can make the cornea more elastic, changing how light waves travel through the eye.
You blink more when talking and less when you are reading. This is why you get tired when reading.
Only two percent of the population have green eyes. The largest concentration of green-eyed peoples is in Ireland, Scotland, and Northern Europe. All races (Asian, African, Caucasian, Pacific Islanders, Arabic, Hispanic, and the indigenous peoples of the Americas) can have green eyes.
All babies are born with blue or brown eyes. Green eyes can take between six months and three years to appear in children.
By three months, our eyes are the same size that they will ever be as the corneas have reached their full width. Human eyes grow rapidly in the womb and for the first three months after birth.
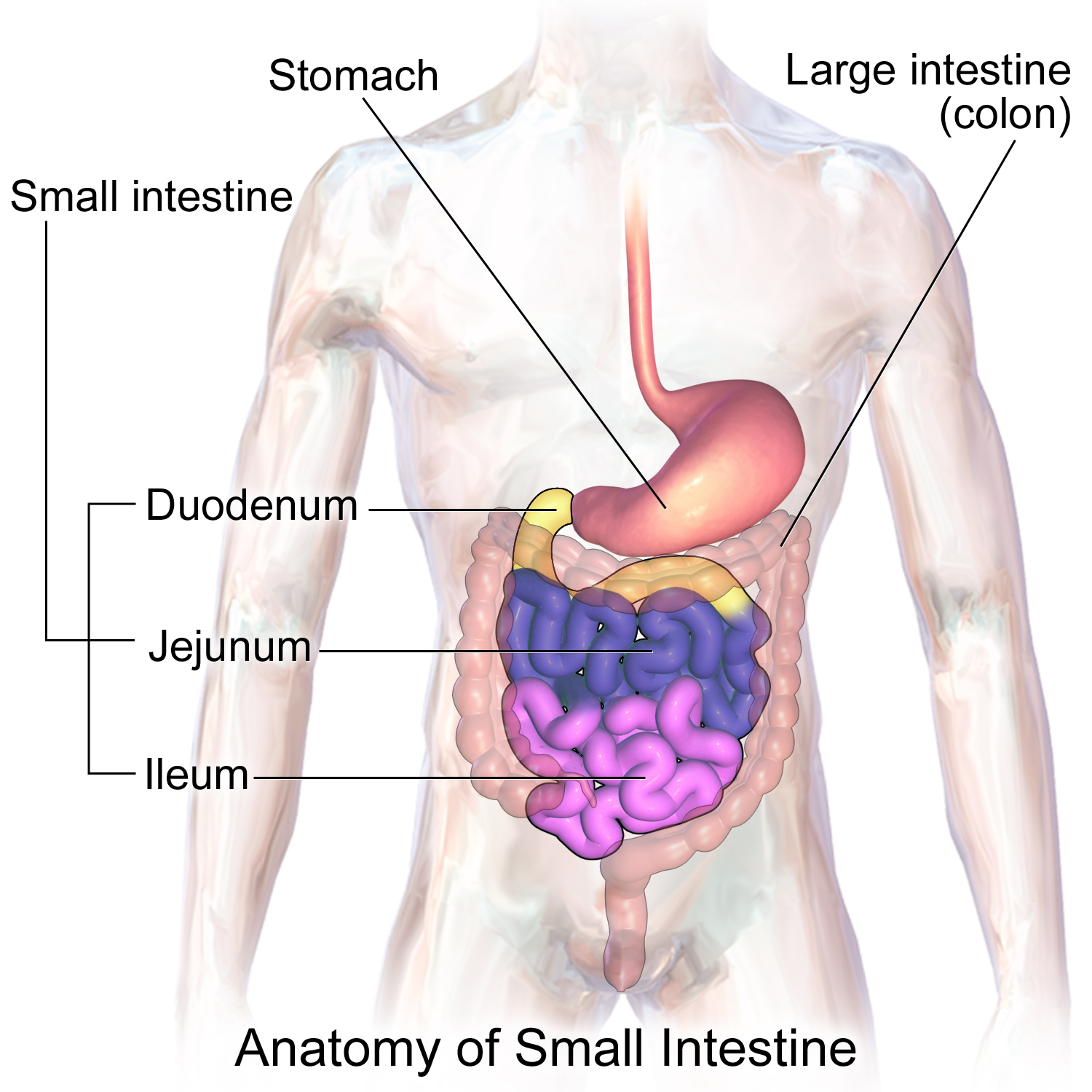
GI Tract
Your sense of smell is around 10000 times more sensitive than your sense of taste.
As well as having unique fingerprints, humans also have unique tongue prints.
It takes the body around 12 hours to completely digest eaten food.
When meds are to be taken “on an empty stomach” that means an hour before or two hours after eating.
You can’t breathe and swallow simultaneously.
On average, your intestines are 25 feet long from end to end. Your small intestine is over 20 feet. And while your large intestine is wider around, it’s only about 5 feet in length.
Your intestines are always moving, a continuous wavy motion called peristalsis. Or when vomiting, reverse-peristalsis.
Stomach acid can melt metal—at least certain metals, such as zinc. Digestive juices in the gut contain hydrochloric acid. They rank just below battery acid on the pH scale.
Your Asymmetrical Body

The two sides of your face are not alike. If you take a photo of your face and divide it down the middle, then replicate each half, the faces look different enough for people to judge one face better looking than the other!
One side of your body is bigger than the other, with bigger hand and foot.
Your left lung is about 10 percent smaller than your right one.
Almost everyone is stronger and more dexterous on one side of their body than the other. Research indicates somewhere between 85% and 90% of the population is right-handed; almost everyone else favors their left hand. Only about 1% of the population is naturally ambidextrous, but it is possible to train one’s non-dominant side to greater strength and ability.
Body Bits and Pieces
All humans share about 99.9% of our DNA with other humans. For comparison, we share 98% with pigs, and 60% with bananas! (thednatests.com)
The extra skin on your elbow, known scientifically as olecranal skin or colloquially at the weenus, is basically nature’s Silly Puddy because there are fewer sensory neurons located there. That means you can keep kneading it all day long, and as hard as you want.
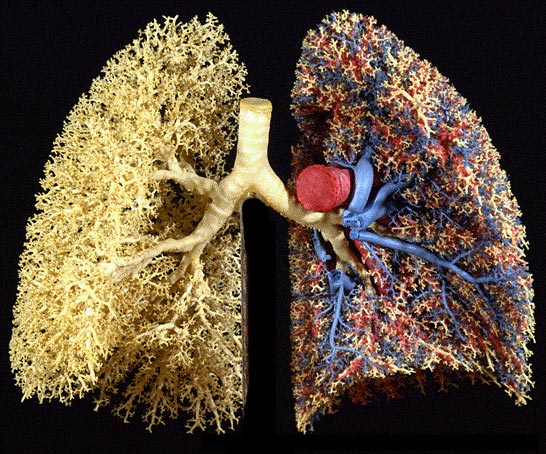
Adult lungs have a surface area of around 70 square meters!
Human teeth are almost as hard as opal. Diamonds have a hardness of 10; teeth are at 5.
You are about 1cm taller in the morning when you first get up than when you go to bed. This is because during the day the soft cartilage between your bones gets squashed and compressed.
Some penises “grow” more than 4 centimeters when aroused. I found nothing about any relationship between this and any aspect of sexual functioning.
Vaginas range from 2.7 to 3.1 inches. The depth while aroused ranges from 4.3 to 4.7 inches.
Men are more sensitive to caffeine; women are more sensitive to alcohol.
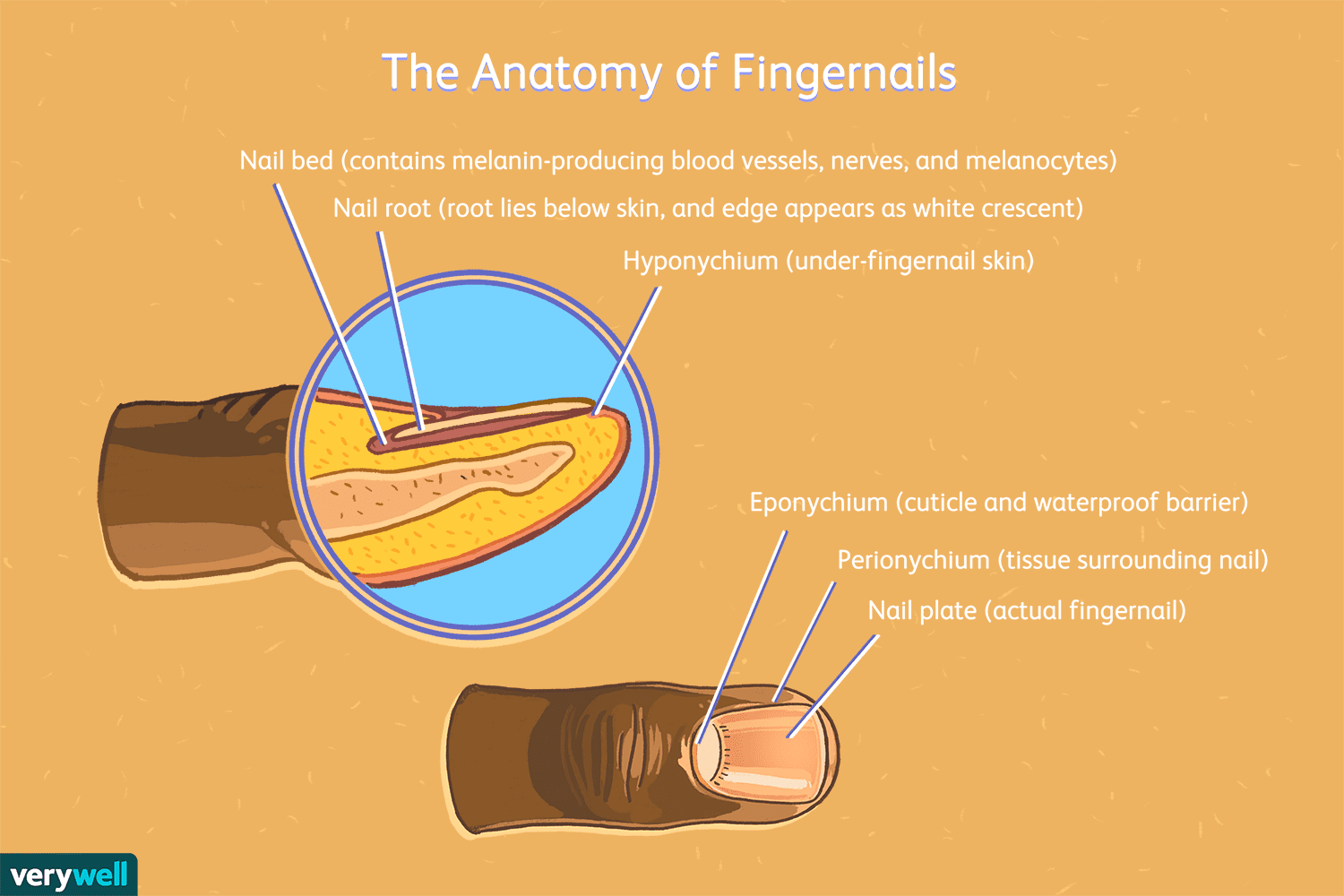
Your fingernails grow three times faster than toenails, explained by the hands having more blood pumping through them. The fingernails on your dominant hand grow faster. In colder weather, nails grow more slowly.
Health changes, such as pregnancy, vitamin deficiencies, menopause, and trauma can show up in your hair and nails. Your hair stylist or manicurist might know you’re pregnant before you do!
The smallest bone found in the human body is located in the middle ear. The stapes (or stirrup) bone is only 2.8 millimeters long.
Human teeth are just as strong as shark teeth.
Spread across their lifetime, most people spend an average of one whole year sitting on the toilet.
Your nose and ears continue growing throughout your entire life.
More Nose Facts
Scientists estimate that the human nose can recognize a trillion different scents!

During pregnancy, one’s sense of smell improves dramatically, possibly the body’s attempt to avoid exposing the fetus to danger.
A human’s scent also changes during pregnancy. Other humans can’t usually detect it, but pets might!
Our bodies give one nostril a break while the other is active – we just don’t know we do it. We naturally tend to alternate breathing from one nostril then the other, which helps keep the air we breathe moist so as not to irritate our lungs.
Identical twins smell the same. No surprise there!
Aging Body
Every new cell is reproduced from the template of our DNA. Therefore, it’s not surprising that this DNA template gets worn away and errors occur as we age. But the aging body is beyond the scope here!
Bottom Line: Know your body well as a path to taking good care of it!