
Today’s blog is written by a fellow writer who wishes to remain anonymous for privacy reasons.
Among the many odd things I’ve done in my life, one that has had the most lasting impact is being a linguistic and cultural ambassador posted to a country that shall remain nameless here. Because of various regional disputes, a massive prison outbreak, less-than-polite national elections and regime changes, and a general culture of aggressiveness, I found myself living in conditions that were much more dangerous than I’d been led to expect.
When I eventually returned home, among the souvenirs and keepsakes I brought back with me, I found in my luggage a serious case of PTSD (post traumatic stress disorder). As Vivian’s blog is for writers and writing, I thought perhaps a guided tour inside the warped and broken mind of a person with PTSD might be of interest to you all.
Please keep hands and arms inside the cart at all times, and don’t feed the negativity gremlins as we go past.
Very Important Disclaimer: Neither Vivian Lawry nor this guest author are psychiatric professionals or are qualified to provide medical assistance. The information contained herein is not intended to be used for diagnostic or treatment purposes in any way, shape, or form.

(It’s actually the Soul Cairn from the Dawnstar plug-in to Elder Scrolls IV: Skyrim by Bethesda.)
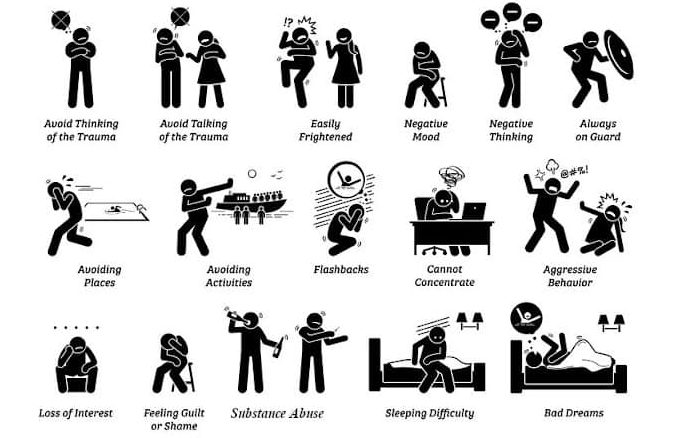
Before the ride begins in earnest, you can look to your left for some basic information about PTSD. The most common association people have with PTSD is of veterans of military combat, but it can result from many different experiences, including natural disasters, abusive relationships, assault (sexual or otherwise), prolonged insecurity, traffic collisions, and so on. People can even develop second-hand PTSD from witnessing these events in other people’s lives. A patient may develop PTSD immediately after an event, but sometimes symptoms don’t appear until well after the event itself.
With all of these possibilities, there are loads of ways in which the inclusion of a character experiencing PTSD can enrich, complicate, drive, or drive, or even resolve your writing. There is a lot of information available about the causes and effects of PTSD, but remember that each case is different. Every person will have different triggers, coping mechanisms, involuntary reactions, etc.
You may notice the cart shaking violently as we enter the tunnel; this is simply the result of uneven neural pathways, nothing to be alarmed about.

As a writer and a reader, I’ve found myself thinking of ways in which my warped thoughts and behaviors could fit in with other common narrative techniques. I have also found some absolutely infuriating stories out there in which a character has a traumatic experience (usually rape or sexual assault) simply so the hero can come to the rescue or to establish a villain as a villain… and victimized character goes right back to skipping through the tulips. Don’t be that writer!
If you look out on either side of the cart, you may be able to make out (through the erratic strobe lights and general gloom) a few of the ways common behaviors of characters with PTSD could be very useful in your writing. Please remember that these are only glimpses from one mind and do not necessarily reflect every patient. Also, hold on to the lap bar as there are some sharp curves coming up.
Unreliable Narrator: What I see and hear is always filtered through the PTSD in my mind. If a story is told from the point of view of a character with PTSD, this is a good way to demonstrate the disconnect from reality. If another character is getting information from a character with PTSD, it could skew everyone’s opinions and affect the plot moving forward.

- Social interactions are a minefield of side-stepping physical attacks (handshakes, hugs, pats on the back).
- Random strangers only ever approach me with violent intentions, such as petting my dog, asking me to reach something off a high shelf, or walking past me on a narrow sidewalk.
- People waiting in parked cars are obviously armed, most likely on the lookout for potential victims.
- Anyone who stands in a doorway must be trying to block the exit or prevent escape.
- An approach from behind must be someone trying to sneak up on me, and anyone who surprises me from behind is an attacker and will be punched.
- This isn’t helped by chronic sleep deprivation giving me the same symptoms as early-onset Alzheimer’s: How can I be trusted to provide accurate information when I lose time and forget everything?
Mistaken Motivations: Objectively, I know there is nothing wrong with mental illness, nor should there be any shame attached. Still, I try to hide it or play it off as no big deal. As a result, family, friends, and strangers all have reason to assume my coping behaviors are something very different. Having a character reveal midway through or near the end of a story that their actions were motivated by coping mechanisms could be a plot twist, a clue for investigators, a reset of other characters’ attitudes, or plenty of other ways of adding narrative interest.

- Friends frequently ask if I’m cold because I can’t stop shaking.
- Constantly scanning for threats and possible exits sometimes makes me look like I’m trying to find someone or looking for an excuse to leave a boring conversation.
- Being hyper-vigilant in general makes me look twitchy, itchy, over-caffeinated, or paranoid, depending on who is providing their opinion.
- My brother thought he’d done something to offend me when I repeatedly moved away from him or left the room when he entered.
- After I repeatedly panicked and cancelled plans at the last minute, many friends thought I was just blowing them off.
- Arriving late to social gatherings, hiding in the corner, and leaving early have all led acquaintances to assume I’m too stuck-up to mingle.
- To make it through particularly important events that I cannot miss, I’ve sometimes taken extra doses of anti-anxiety medication. My slurred speech, unfocused gaze, less than ideal balance, and inability to follow conversation looks an awful lot like I’ve shown up to the baptism or wedding drunk as a skunk.
- I escape to the bathroom a lot when things get overwhelming, sometimes for extended periods of time. Most of my family now thinks I have severe digestive issues.
Affects in My Life: In order to be diagnosed as a disorder (the D in PTSD) a patient must have symptoms severe enough to disrupt their ability to live a normal life. A character who develops PTSD midway through a narrative would almost certainly show changes in behaviors. These are some of mine.

- Chronic insomnia and nightmares: Years later, I still sleep in a separate room from my spouse, with the lights on, with distracting or soothing music playing… and I still manage to wake the household at least once a month by screaming in my sleep.
- My ability to concentrate and complete tasks on time severely impacted my job. Twice, I responded to a coworker trying to get my attention by panicking and attacking them. Going into the office grew increasingly difficult as it became harder to leave the house. I am now unemployed.
- Weeks at a time go by when I cannot leave my house, even to go into the backyard. I feel threatened every time I open the door.
- Side effects from different medications I’ve tried have included weight gain, headaches, heartburn, memory loss, drowsiness, etc. etc. etc. ad nauseam. These could also be examples of mistaken motivations!
- I no longer participate in hobbies I once did, especially anything that involves leaving the house or interacting with other people.
- Suicide and suicide attempts are very common among patients with PTSD.
Anxiety Attacks, Panic Attacks, and Flashbacks: These can be triggered by almost anything, depending on the person and the situation. Smelling cigarette smoke, walking on an icy sidewalk, being in a room of people speaking another language I only halfway understand… any of these can send me spiraling. Being under stress increases the chance that something will hit that switch.
Ladies and Gentlemen, we’d like to remind you at this time that motion sickness bags can be found under your seats and to hold on tightly.

- Anxiety or Panic Attack: It’s really bizarre to be terrified and not know why. Why is my heart racing? Why can’t I breathe? Why can I not stop screaming? When I have an anxiety attack, I don’t think rationally but I can speak and respond to people around me. When I have a panic attack, it feels like I’m about to die. I can’t feel anything but the absolute terror that completely takes over my body. Usually, I am able to leave a situation when I feel one of these about to happen so that I can mentally implode in the peace and quiet of a public urinal.
- Flashback: These are even more bizarre. Anxiety attacks often segue into flashbacks. I am completely unaware of my surroundings and respond to threats that are long gone. I’ll switch languages to talk to people who aren’t there; I’ll be able to smell the food or feel the cold from specific memories. Sometimes, I have flashbacks that aren’t tied to precise events, more an amalgamation of similar threats that get lumped together in my head. It’s very embarrassing to come out of it and realize that I’m hiding behind a clothes rack in Target, desperately fighting off the attack of a stiff coat sleeve.
Treatment Options: There are many different types of treatments for PTSD, with varying degrees of accessibility, cost, success, and side effects. I’ve tried just about everything: some worked, some did not, some worked at first and then stopped. I can’t stress enough that every person will respond differently to different treatments. The information here is simply what undergoing the treatments felt like for me.

- Therapy Animal: My dog trained himself to be a therapy dog because he was just that awesome. Before I was eventually laid off, my boss let me bring my dog into the office with me. He learned to impose himself between me and anyone getting too close to my personal space. When I had anxiety attacks, he’d put his head in my lap and nudge my hand until I pet him. Focusing on the feeling of his fur, his cold nose, his super stinky breath worked to calm me down and remind me that I was safe. He passed away in April, and it felt like going through all the trauma again.
- TMS (Trans-Cranial Magnetic Stimulation): It felt a bit like sitting in the dentist’s chair while a woodpecker tapped on my head. I went every day for three months, and the only side effect was a minor headache when I first started.
- EMDR (Eye Movement Desensitization and Reprocessing): My eyesight is so bad that I couldn’t do the actual eye movement part of it; I held a buzzer in each hand and felt the vibrations in alternating hands at different speeds. In each session, I relived particularly traumatic events over and over while the therapist guided me through sense memories and varied the speed of the buzzing. By the time the hour was up, I was usually an exhausted, damp, shaking mess running to the bathroom to vomit.
- Medication: I think by now I’ve tried every different medication type on the market. I can’t even pronounce most of them and have to stutter and hope at the pharmacy. Most gave some relief for a little while and then stopped working.
- There is now a way in which doctors can send a sample of your DNA to a lab, where people in white coats and shiny goggles can magically determine which medicines will or won’t work for you. I have no idea how they do it; I assume it involves cauldrons and eyes or tails of newts.
- Ketamine: I was very hesitant to try this method because there have been so few long-term studies. When I started, I went in every day for a week and a half. After that, I went in every three to four weeks depending on how the doctor thinks I’m doing. Ketamine treatment is available through aerosol or intravenously. I sit in a comfy chair with a needle in my arm for about an hour while geometry loses all meaning and everything becomes either fascinating or hilarious. Everything in the universe swirls in front of my face, and the feeling of my hair is the most amazing sensation I can remember. According to the nurse, I tend to wax rhapsodic about how much I love every person who comes through the door. For some reason, they won’t let me drive afterwards!
- Healing Crystals/ Salt Lamps/ Essential Oils: I had a lumpy pillow, a pink wall, and everything tasted like lavender.
- PTSD is expensive!

I hope you’ve enjoyed this tour through the mess inside my head. Please wait for the ride to come to a complete stop before unbuckling safety harnesses. Be sure to gather all personal items and take them with you as you exit down the ramp to your right. Don’t forget to check the photo booth for a hilarious souvenir memento of your trip. You can also find resources for actual help; as I’m sure you remember, this has just been an example of some personal experiences for your writing toolbox.
- NAMI (National Alliance for Mental Health) PTSD
- APNA (American Psychiatric Nurses Association) PTSD Toolkit
- PTSD Alliance
