Energy is always high when I arrive at Nimrod on Sunday: getting settled, reuniting with friends, meeting the new writers, and getting the schedule for the week ahead.



I was in Square House again this year, my favorite room! It’s downstairs, dim, and I know where my things will fit and how many extension cords I’ll need.


Monday through Thursday at Nimrod is intense: focused writing, talk with fellow writers—who often ask how your work is going, which certainly reinforces that focus and productivity are expected and rewarded—reading every day for workshop, sharing opinions with other readers, then listening to the 8:00 readers after dinner…
All of this happening across varied genres leaves me feeling worn. I suspect others do as well.

So an open day on Friday was cherished! I walked in sunshine for the first time.
It’s also a chance to tie things up. I (finally) turned to to the reference Cathy Hankla had given me on Monday! Unfortunately, I could not send off “Repair or Redecorate?” because my computer went all wonky. The touch-pad didn’t control the cursor. Damn! But at least it’s ready to go. I started packing to leave on Saturday.

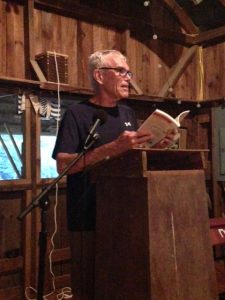
I got a photo of Thursday’s readers on Friday evening, in the course of a most entertaining variety show! This was new to my years at Nimrod. Kristy Bell did an incredible job as MC! We had multiple readings of poetry, fiction, memoir, and all the other genre’s represented here, up and down the emotional spectrum. But we also had musical interludes!


Terry Dolson accompanied Judy Bice, Amelia Williams, and Sheri Reynolds while the rest of us joined in as well as we could on such classics as “Country Road” and “Bobbie McGee.” I’m here to tell you, Sheri Williams does a mean Janis Joplin!


Most year I’ve gone to the Jefferson Baths. This year, I mourn missing it. But several of us had accepted a neighbor’s invitation for drinks and a visit to the champion sycamore tree: 10 feet across, 33 feet around. It was good viewing and very good scotch!
Every year we take a group picture. This one came was Saturday morning, just after breakfast.

Unfortunately, several people left on Friday. Oh, sigh. Maybe next year!


By 10:00 Saturday morning, Frances Burch and I were on the road. We followed our usual routine: we stopped in Crozet, Virginia for shopping at Over the Moon Bookstore and lunch at Crozet Pizza. For the first time ever, we had their specialty pizza that is a white base, topped with herbs, summer squash, and peanuts! It was excellent.
I was home by 3:00, but Nimrod lingers. There’s always a long re-entry time!
Nimrod Hall, established in 1783, has been providing summer respite from everyday stress since 1906. It has been operating as an artist and writer colony for over 25 years. The Nimrod Hall Summer Arts Program is a non-competitive, inspirational environment for artists to create without the distractions of everyday life.