There is a whole cadre—Heidegger (1889-1976) arguably the most famous—who argue that being-with-others is part of the “structure of human existence.” In other words, we are hard-wired to socialize. Whether you believe that or not, there are a gazillion (by actual count) studies that have found isolation to be harmful to humans, both physically and psychologically.
Litter of Puppies
(Editor’s note: Including photographs of isolated and lonely people was too depressing, so I invite you to enjoy these photos of animals not social distancing instead.)
For writers, bad is good
Pod of Dolphins
How bad is it? Some researchers posit that social isolation and loneliness are twice as harmful as obesity. Others compare the effects on mortality to be equal to smoking 15 cigarettes per day. Others say the magnitude of risk is right up there with physical inactivity and lack of access to health care.
N.B. Degrees or levels of isolation are difficult to define and measure. Perceived isolation is what produces feelings of loneliness. In many ways, it is easier to studysocial isolation, though they are closely linked.
Pandemonium of Parrots
As a writer, the first question is, “Why is your character isolated?” Your options may be more numerous than you think. Here are a few examples.
Death of a loved one
Divorce
Move to a new place
Researcher in isolated places, like Antarctica
Mission/mission training, e.g., astronauts
Immune compromised
Leap of Leopards
A child/infant in understaffed orphanage
Being shunned for any reason
Behavior
Appearance
Membership in a marginalized subgroup
Medical quarantine
As a form of torture
Solitary confinement in prison (currently about 80,000 in the U.S. each year)
Tower of Giraffes
The second set of questions for a writer:
How complete is the isolation?
How long does it last?
Is it repeated?
In general, the more complete the isolation, the longer it lasts, and repetition all increase the number and seriousness of the effects.
Mob of Kangaroos
The third question is, which effects will your character display?
Parliament of Owls
Fatigue
Insomnia
Headaches
Sweaty palms
Heart palpitations
Lowered immunity
Increased inflammation
Trembling
Diarrhea
Stomach pains
Lack of appetite
Drastic weight loss
Stand of Flamingos
Muscle pains (esp. neck and back)
Oversensitivity to sensory stimuli
Difficulty concentrating
Dizziness
Distorted sense of time
Severe boredom
Impaired memory
Inability to think coherently
Apathy
Conspiracy of Lemurs
Anxiety
Panic
Feelings of inadequacy
Feelings of inferiority
Irritability
Withdrawal
Rage/anger/aggression
Confusion
Paranoia
Depression
Suicidal thoughts
Hallucinations
Many of these effects mimic PTSD and, like PTSD, can last for years after the event.
Bale of Turtles
In the last couple of months, researchers are finding that COVID-19 isolation tends to evoke one of two responses.
Smack of Jellyfish
Those who hunker down and enjoy it—take it as a time to relax, read, bake, pursue a hobby, accomplish things around the house. In short, they’re getting along fine.
But for others—especially extroverts—the isolation can be harmful to both mind and body.
Not surprisingly, the effects of COVID-19 isolation are many of the same effects as other reasons for isolation.
Drift of Pigs
Boredom
Lethargy
Anxiety
Depression
Distorted sense of time
Poor sleep quality
Develop or increase unhealthy habits
Dr. Samantha Brooks wrote in The Lancet: “A huge factor in the negative psychological impact [of isolation] seems to be confusion about what’s going on, not having clear guidelines, or getting different messages from different organizations.” In addition, not knowing how long isolation will last exacerbates the negative effects of isolation. Think of the current differences within the U.S. and how similar circumstances could be applied to a fictional setting.
Obstinacy of Buffalo
People who are at increased risk from COVID-19 isolation are those at heightened risk for social isolation in the first place:
Gang of Elk
Older adults, especially with physical limitations and/or poor family support
Men who didn’t develop social networks outside work
Being non-white is a bigger risk factor than sex
Lower income people who may not afford the technology for distance socializing
Anyone who is marginalized (LGBTQ, survivor of domestic abuse, living in an isolated rural area)
Today’s blog is written by a fellow writer who wishes to remain anonymous for privacy reasons.
Among the many odd things I’ve done in my life, one that has had the most lasting impact is being a linguistic and cultural ambassador posted to a country that shall remain nameless here. Because of various regional disputes, a massive prison outbreak, less-than-polite national elections and regime changes, and a general culture of aggressiveness, I found myself living in conditions that were much more dangerous than I’d been led to expect.
When I eventually returned home, among the souvenirs and keepsakes I brought back with me, I found in my luggage a serious case of PTSD (post traumatic stress disorder). As Vivian’s blog is for writers and writing, I thought perhaps a guided tour inside the warped and broken mind of a person with PTSD might be of interest to you all.
Please keep hands and arms inside the cart at all times, and don’t feed the negativity gremlins as we go past.
Very Important Disclaimer: Neither Vivian Lawry nor this guest author are psychiatric professionals or are qualified to provide medical assistance. The information contained herein is not intended to be used for diagnostic or treatment purposes in any way, shape, or form.
This is basically what the inside of my mind looks like. (It’s actually the Soul Cairn from the Dawnstar plug-in to Elder Scrolls IV: Skyrim by Bethesda.)
Before the ride begins in earnest, you can look to your left for some basic information about PTSD. The most common association people have with PTSD is of veterans of military combat, but it can result from many different experiences, including natural disasters, abusive relationships, assault (sexual or otherwise), prolonged insecurity, traffic collisions, and so on. People can even develop second-hand PTSD from witnessing these events in other people’s lives. A patient may develop PTSD immediately after an event, but sometimes symptoms don’t appear until well after the event itself.
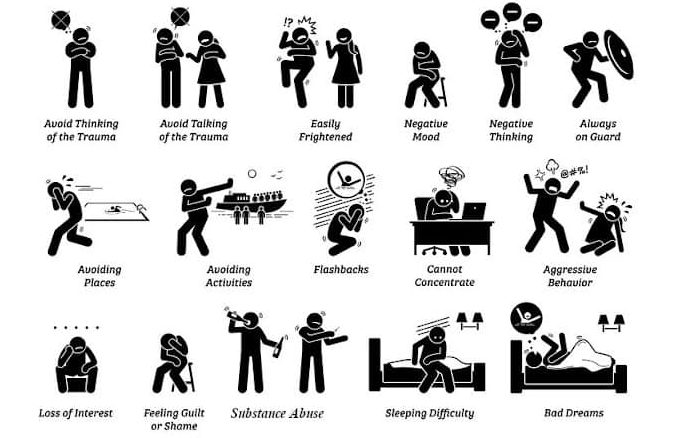
Common symptoms of PTSD. As soon as I can cultivate a substance abuse problem, I’ll have BINGO! (That’s how it works, right?)
With all of these possibilities, there are loads of ways in which the inclusion of a character experiencing PTSD can enrich, complicate, drive, or drive, or even resolve your writing. There is a lot of information available about the causes and effects of PTSD, but remember that each case is different. Every person will have different triggers, coping mechanisms, involuntary reactions, etc.
You may notice the cart shaking violently as we enter the tunnel; this is simply the result of uneven neural pathways, nothing to be alarmed about.
As a writer and a reader, I’ve found myself thinking of ways in which my warped thoughts and behaviors could fit in with other common narrative techniques. I have also found some absolutely infuriating stories out there in which a character has a traumatic experience (usually rape or sexual assault) simply so the hero can come to the rescue or to establish a villain as a villain… and victimized character goes right back to skipping through the tulips. Don’t be that writer!
If you look out on either side of the cart, you may be able to make out (through the erratic strobe lights and general gloom) a few of the ways common behaviors of characters with PTSD could be very useful in your writing. Please remember that these are only glimpses from one mind and do not necessarily reflect every patient. Also, hold on to the lap bar as there are some sharp curves coming up.
Unreliable Narrator: What I see and hear is always filtered through the PTSD in my mind. If a story is told from the point of view of a character with PTSD, this is a good way to demonstrate the disconnect from reality. If another character is getting information from a character with PTSD, it could skew everyone’s opinions and affect the plot moving forward.
What it feels like to walk down the street.
Social interactions are a minefield of side-stepping physical attacks (handshakes, hugs, pats on the back).
Random strangers only ever approach me with violent intentions, such as petting my dog, asking me to reach something off a high shelf, or walking past me on a narrow sidewalk.
People waiting in parked cars are obviously armed, most likely on the lookout for potential victims.
Anyone who stands in a doorway must be trying to block the exit or prevent escape.
An approach from behind must be someone trying to sneak up on me, and anyone who surprises me from behind is an attacker and will be punched.
This isn’t helped by chronic sleep deprivation giving me the same symptoms as early-onset Alzheimer’s: How can I be trusted to provide accurate information when I lose time and forget everything?
Mistaken Motivations: Objectively, I know there is nothing wrong with mental illness, nor should there be any shame attached. Still, I try to hide it or play it off as no big deal. As a result, family, friends, and strangers all have reason to assume my coping behaviors are something very different. Having a character reveal midway through or near the end of a story that their actions were motivated by coping mechanisms could be a plot twist, a clue for investigators, a reset of other characters’ attitudes, or plenty of other ways of adding narrative interest.
Friends frequently ask if I’m cold because I can’t stop shaking.
Constantly scanning for threats and possible exits sometimes makes me look like I’m trying to find someone or looking for an excuse to leave a boring conversation.
Being hyper-vigilant in general makes me look twitchy, itchy, over-caffeinated, or paranoid, depending on who is providing their opinion.
My brother thought he’d done something to offend me when I repeatedly moved away from him or left the room when he entered.
After I repeatedly panicked and cancelled plans at the last minute, many friends thought I was just blowing them off.
Arriving late to social gatherings, hiding in the corner, and leaving early have all led acquaintances to assume I’m too stuck-up to mingle.
To make it through particularly important events that I cannot miss, I’ve sometimes taken extra doses of anti-anxiety medication. My slurred speech, unfocused gaze, less than ideal balance, and inability to follow conversation looks an awful lot like I’ve shown up to the baptism or wedding drunk as a skunk.
I escape to the bathroom a lot when things get overwhelming, sometimes for extended periods of time. Most of my family now thinks I have severe digestive issues.
Affects in My Life: In order to be diagnosed as a disorder (the D in PTSD) a patient must have symptoms severe enough to disrupt their ability to live a normal life. A character who develops PTSD midway through a narrative would almost certainly show changes in behaviors. These are some of mine.
This is perfectly normal.
Chronic insomnia and nightmares: Years later, I still sleep in a separate room from my spouse, with the lights on, with distracting or soothing music playing… and I still manage to wake the household at least once a month by screaming in my sleep.
My ability to concentrate and complete tasks on time severely impacted my job. Twice, I responded to a coworker trying to get my attention by panicking and attacking them. Going into the office grew increasingly difficult as it became harder to leave the house. I am now unemployed.
Weeks at a time go by when I cannot leave my house, even to go into the backyard. I feel threatened every time I open the door.
Side effects from different medications I’ve tried have included weight gain, headaches, heartburn, memory loss, drowsiness, etc. etc. etc. ad nauseam. These could also be examples of mistaken motivations!
I no longer participate in hobbies I once did, especially anything that involves leaving the house or interacting with other people.
Suicide and suicide attempts are very common among patients with PTSD.
Anxiety Attacks, Panic Attacks, and Flashbacks: These can be triggered by almost anything, depending on the person and the situation. Smelling cigarette smoke, walking on an icy sidewalk, being in a room of people speaking another language I only halfway understand… any of these can send me spiraling. Being under stress increases the chance that something will hit that switch.
Ladies and Gentlemen, we’d like to remind you at this time that motion sickness bags can be found under your seats and to hold on tightly.
It doesn’t look quite as cute when I do it.
Anxiety or Panic Attack: It’s really bizarre to be terrified and not know why. Why is my heart racing? Why can’t I breathe? Why can I not stop screaming? When I have an anxiety attack, I don’t think rationally but I can speak and respond to people around me. When I have a panic attack, it feels like I’m about to die. I can’t feel anything but the absolute terror that completely takes over my body. Usually, I am able to leave a situation when I feel one of these about to happen so that I can mentally implode in the peace and quiet of a public urinal.
Flashback: These are even more bizarre. Anxiety attacks often segue into flashbacks. I am completely unaware of my surroundings and respond to threats that are long gone. I’ll switch languages to talk to people who aren’t there; I’ll be able to smell the food or feel the cold from specific memories. Sometimes, I have flashbacks that aren’t tied to precise events, more an amalgamation of similar threats that get lumped together in my head. It’s very embarrassing to come out of it and realize that I’m hiding behind a clothes rack in Target, desperately fighting off the attack of a stiff coat sleeve.
Treatment Options: There are many different types of treatments for PTSD, with varying degrees of accessibility, cost, success, and side effects. I’ve tried just about everything: some worked, some did not, some worked at first and then stopped. I can’t stress enough that every person will respond differently to different treatments. The information here is simply what undergoing the treatments felt like for me.
He still can’t change the printer cartridges.
Therapy Animal: My dog trained himself to be a therapy dog because he was just that awesome. Before I was eventually laid off, my boss let me bring my dog into the office with me. He learned to impose himself between me and anyone getting too close to my personal space. When I had anxiety attacks, he’d put his head in my lap and nudge my hand until I pet him. Focusing on the feeling of his fur, his cold nose, his super stinky breath worked to calm me down and remind me that I was safe. He passed away in April, and it felt like going through all the trauma again.
TMS (Trans-Cranial Magnetic Stimulation): It felt a bit like sitting in the dentist’s chair while a woodpecker tapped on my head. I went every day for three months, and the only side effect was a minor headache when I first started.
EMDR (Eye Movement Desensitization and Reprocessing): My eyesight is so bad that I couldn’t do the actual eye movement part of it; I held a buzzer in each hand and felt the vibrations in alternating hands at different speeds. In each session, I relived particularly traumatic events over and over while the therapist guided me through sense memories and varied the speed of the buzzing. By the time the hour was up, I was usually an exhausted, damp, shaking mess running to the bathroom to vomit.
Medication: I think by now I’ve tried every different medication type on the market. I can’t even pronounce most of them and have to stutter and hope at the pharmacy. Most gave some relief for a little while and then stopped working.
There is now a way in which doctors can send a sample of your DNA to a lab, where people in white coats and shiny goggles can magically determine which medicines will or won’t work for you. I have no idea how they do it; I assume it involves cauldrons and eyes or tails of newts.
Ketamine: I was very hesitant to try this method because there have been so few long-term studies. When I started, I went in every day for a week and a half. After that, I went in every three to four weeks depending on how the doctor thinks I’m doing. Ketamine treatment is available through aerosol or intravenously. I sit in a comfy chair with a needle in my arm for about an hour while geometry loses all meaning and everything becomes either fascinating or hilarious. Everything in the universe swirls in front of my face, and the feeling of my hair is the most amazing sensation I can remember. According to the nurse, I tend to wax rhapsodic about how much I love every person who comes through the door. For some reason, they won’t let me drive afterwards!
Healing Crystals/ Salt Lamps/ Essential Oils: I had a lumpy pillow, a pink wall, and everything tasted like lavender.
PTSD is expensive!
I hope you’ve enjoyed this tour through the mess inside my head. Please wait for the ride to come to a complete stop before unbuckling safety harnesses. Be sure to gather all personal items and take them with you as you exit down the ramp to your right. Don’t forget to check the photo booth for a hilarious souvenir memento of your trip. You can also find resources for actual help; as I’m sure you remember, this has just been an example of some personal experiences for your writing toolbox.
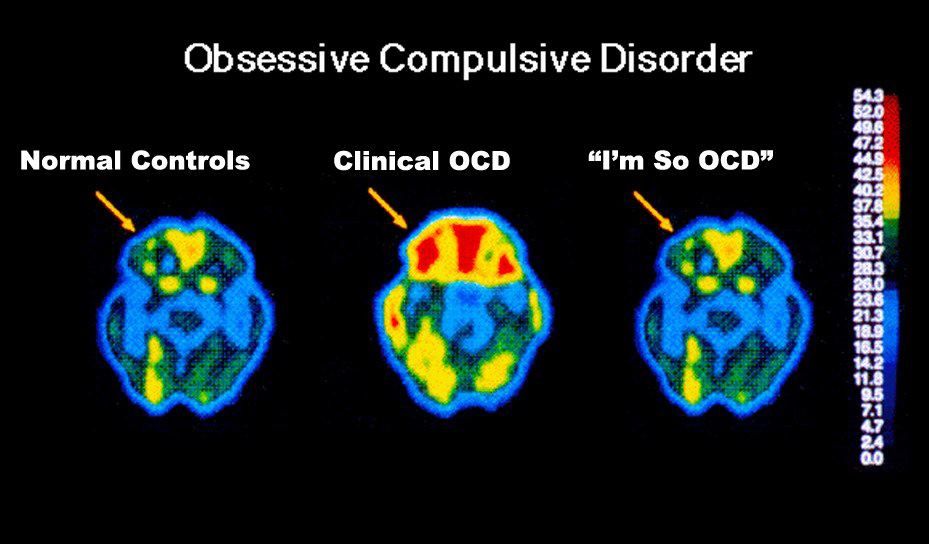
OCD, like love and hate, is a label thrown around pretty loosely, often for humorous effect. People with fixations on organization, precise routines, hygiene, perfectionism, etc. are frequently referred to as “acting so OCD” or “showing their inner OCD.” Marketing campaigns turn OCD into a punchline to sell products like Obsessive Christmas Disorder pajamas or Khlo-CD organizational apps.
Hilarious, no?
There is a significant difference between people with odd quirks and people who have a diagnosable mental illness. Both can be useful characters for writers, albeit in very different ways. Characters who have fixations, quirks, rituals, or habits that interrupt a scene or cause awkward situations can be a source of amusement for writers. Characters who actually have Obsessive Compulsive Disorder can be a source of tension, tragedy, or demonstrated compassion for writers, but the actual mental illness is not amusing.
Confusing retail workers is a sign of having too much time on one’s hands rather than having a debilitating mental illness. (Disclaimer: This blog is not affiliated with any retail chain or candy brand.)
Obsessive-Compulsive Disorder is a common, chronic, and long-lasting disorder in which a person has uncontrollable, recurring thoughts (obsessions) and/or behaviors (compulsions that s/he feels the urge to repeat over and over). The line between having a personality quirks and a mental disorder can be hard to find, but it generally comes down to quality of life. Dr. Steven Brodsky points out that actual OCD will “impair social or occupational function or involve frequent excessive distress” in the lives of those suffering from it.
Obsessions—repeated thoughts, urges, or mental images—are private, and thus no one knows about them but the person unless they’re talked about. These uncomfortable thoughts cause anxiety.
Compulsions are typically (but not always) public, as is any behavior that happens the presence of others. The repetitive behaviors are an attempt to deal with the anxiety the obsessive thoughts create.
Could you benefit from an O and/or C character? Although people/characters can exhibit symptoms of obsessions, compulsions, or both, thoughts and behaviors typically occur together. See the end of this blog for specific prompts.
Consider Monk, The Big Bang Theory, and Friends. All three shows feature characters who exhibit signs of obsessions and compulsive behaviors, usually to the sound of the laugh-track. All three characters are referred to by others as “obsessive,” “OCD,” or some variation thereof, but none experience the pain that comes along with mental illness (which I can only imagine would be heightened by hearing laughing crowds).
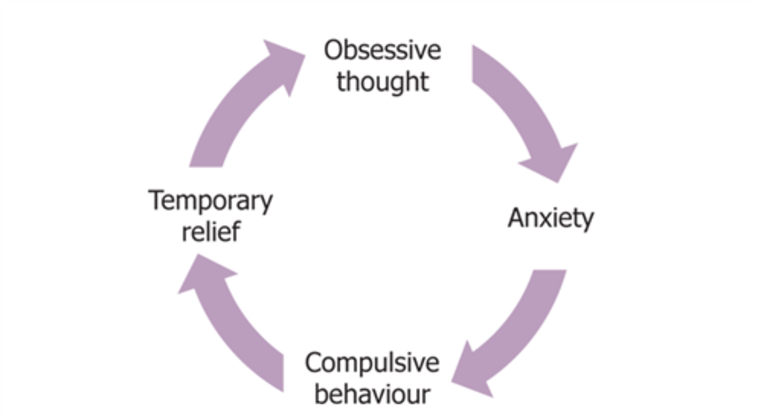
Obsessive thoughts and compulsive behaviors become part of a vicious cycle in the minds of people with OCD. Most people with OCD realize that their thoughts and behaviors are irrational, but they are unable to break the cycle. Children often don’t perceive their abnormality; symptoms are noticed by parents and/or teachers.
In contrast, “neat freaks” and people with fixations often enjoy performing the behavior in question (such as alphabetizing books), enjoy the results (such as having a tidy apartment), have had the behavior drummed into them (such as rewinding video tapes after working at Blockbuster for years [I realize that I’m dating myself]), or out of practical necessity.
An over-organized closet may be a necessity for a working mother of two, saving endless headaches on school mornings.
Most People with OCD Fall Into One of the Following Categories (in no particular order)
Washers are afraid of contamination. They usually have cleaning or hand-washing compulsions. Many refuse to wear anything someone else has worn, take their own sheets to hotels/motels, etc.
Washing your hands before and after eating is just being extra hygienic; washing your hands until they are raw and cracked is a probable sign of OCD.
Checkers repeatedly check things (motion-sensor lights turned on, car locked) they associate with safety. They might keep guns or other weapons that are checked for accessibility, condition, etc.
Jiggling the door handle after locking it could be a funny quirk; checking the lights, the thermostat, the window latches, and everything else repeatedly until you’re late for work is a sign of unhealthy compulsion.
Doubters and sinners are afraid that if everything isn’t perfect or done just so something terrible will happen or they will be punished. Dressing, undressing, bathing, eating must be done in precisely the same way, for example. Or furniture cannot be moved. Cars must always be the same make.
This can also take the form of rituals that must be completed regardless of convenience or safety, such as always taking seven steps at a time or touching every surface in a room, including the hot stove top.
Counters and arrangers are obsessed with order and symmetry, perhaps including superstitions about certain numbers, colors, or arrangements. For example, counting all the angles in a room, or the number of furniture legs.
Being unable to enter rooms painted blue or walk without counting sets of four steps sounds amusing… until the door out of the burning house is in a blue room five steps away.
Hoarders keep things they neither need nor use. They fear that getting rid of anything will cause something bad to happen, or it will be needed later. These people are often co-diagnosed with other disorders, such as depression, PTSD, ADHD, compulsive buying, or kleptomania. They might engage in skin-picking.
OCD symptoms may come and go over time. Added stressors increase symptoms.
It’s a vicious circle: obsessive thoughts trigger anxiety, which leads to compulsive behavior to try to curb the anxiety, and the behavior is followed by temporary relief.
Writers consider the following:
A person who actually is threatened in some way while others dismiss the anxiety and precautions as being silly fixations
A character whose compulsive behaviors are humorous and the source of derision/ joking among coworkers or friends/ acquaintances
A character whose compulsive behaviors embarrass children or other family members
A person whose compulsive behaviors put the family in financial jeopardy
A person whose compulsive behavior leads neighbors, classmates, and others to ostracize the person AND his/her family
A character who keeps obsessive thoughts private, doesn’t act on them, and the strain leads to withdrawal from intimate relationships
A character whose obsessions get them into medical or legal trouble
A character whose OCD has become so severe that they are unable to leave the house or keep a job
Bottom line for writers: OCD characters can provide tension, tragedy, and plot development; fixated or quirky characters can provide humor. There is a big difference.
Who doesn’t want people to be safe in their homes? Writers! Injury and death are bread and butter for writer. But even if you aren’t a writer, you should read what follows to help protect yourself and your family from these dangers. I’ll start with the more innocuous or less common hazards. Consider the following.
Accidents
Extension cords:
Extension cords cause about 3300 residential fires each year, injuring or killing more than 300 people. If used continuously, insulation deteriorates fast. Even if not in use, extension cords left lying around can present a hanging or choking hazard for children.
They are actually little balls of pesticide. They can cause a breakdown in red blood cells in children with certain genetic diseases (such as Glucose-6 Phosphate Dehydrogenase Deficiency). In addition, exposure can lead to nausea, vomiting, dizziness, fatigue, headaches, and eye and nasal irritation in humans; kidney and liver damage in pets.
Mothballs can be huffed for a brief high caused by the dichlorobenzene or naphthalene, either of which can lead to addiction, brain damage, and death.
NB, not as common in homes as they used to be.
Humidifiers:
Water left to sit in the humidifier for long periods of time become rife with mold spores, fungus, and bacteria.
Ultrasonic humidifiers can be particularly dangerous, because they aerosolize and disperse as a mist everything that might be in water, including chemicals, minerals, bacteria, and mold.
Pressed wood:
Products made from hardwood plywood, particleboard, or fiberboard are often made with formaldehyde. Prolonged exposure can cause watery eyes, burns ins eyes and/or throat, asthma attacks, and cancer in animals and perhaps in humans.
This little party crasher might be hanging around in your living room.
Carpeting:
New carpet can emit potentially dangerous chemicals called volatile organic components. Any carpet can trap dust mites, pet dander, mold, dirt, etc., all of which are hard on respiratory systems.
Lead:
Lead poisoning occurs when lead builds up in the body, often over months or years. Even small amounts of lead can cause serious health problems.
Lead paint was commonly used in homes built before 1978. Toys and furniture made in countries with less stringent health safety protocols may still be covered in lead paint.
In very old houses (1920s and earlier), original plumbing may be made of lead, causing all the water coming into the house to be contaminated.
Children younger than 6 years are especially vulnerable to lead poisoning, which can severely affect mental and physical development. At very high levels, lead poisoning can be fatal.
Polycarbonate plastics:
This is most dangerous when used to make food storage containers. The problem is the degradation of the chemical bisphenol (BPA) when it comes in contact with water. Health agencies have gone back and forth on the dangers of BPA, but studies have linked it to disruptions in the endocrine system and ultimately to cancer.
Flame retardants, which seem like they are good things, actually have a downside: most contain toxins that have been linked to cancer, birth defects, diminished I.Q., and other problems.
Space heaters:
More than 25,000 home fires every year, especially those that don’t have an emergency tip-over feature and don’t have eating element guards. They are especially dangerous for children and pets.
Houseplants:
Many common varieties of houseplants, kept for air purification, beautification, or even medicinal purposes, are toxic to humans and animals in the wrong context. While most adults can be trusted not to eat the leaves, chew on the roots, or drink the water from random pots around the house, the same may not be true of children and pets.
Philodendron, peace lilies, oleanders, pothos, and caladium are among the most common houseplants, and all are poisonous to humans and pets.
Christmas trees:
The combination of dry winter air, hot light bulbs, and paper or wooden ornaments make for a perfect storm of conflagration. Add in tinsel, paper-wrapped boxes, and the tendency of many families to leave the tree lights on overnight, and it’s surprising that there aren’t even more house fires and deaths every year.
Fires caused by Christmas trees are among the most deadly house fires: approximately one out of every 34 home fires caused by a Christmas tree results in a death.
Decorative or scented holiday candles can be quite deadly as well. The top three days for fires caused by unsafe candles are Christmas Eve, Christmas Day, and New Year’s Day.
Asbestos removal is a very complicated process.
Other possibilities:
Asbestos, carbon dioxide, radon, cuts, slip and fall accidents, carbon monoxide, unbalanced heavy furniture, stairs, throw rugs, icy walkways, mixing up the sugar and the rat poison…
I’m not sure if this counts as a home injury or a vehicle accident.
Leading Causes of Unintentional Home Injury
Children and the elderly are at greatest risk.
Falls: more than 40% of nonfatal home injuries; more than one third of unintentional home injury deaths.
Poisoning: most unintentional home poisoning deaths are of adults and are caused by heroin, appetite suppressants, pain killers, and narcotics. Other frequent poisons are amphetamines, caffeine, antidepressants, alcohol, motor vehicle exhaust gas, etc.
Children under 5 have the highest rates of non-fatal poisoning, often from exposure to substances not typically thoughts of as poisonous.
“Hidden” poisons can be found in household and cleaning products; personal care and beauty products; medicines, vitamins, plants, and lead paint.
Fires/burns: the third leading cause of unintentional home injury and death. Death rate is highest among senior citizens and —again—children under five. A huge percentage of burns are from hot water. Depending on water heater settings, tap water can be hot enough to cause second-degree burns.
Choking and suffocation: the leading cause of death for infants under the age of one. An average of one child a month dies due to strangulation from a window chord.
Drowning/submersion: 80% are children under age 4, mostly in bathtubs and swimming pools. Because they are top-heavy, a toddler can drown in a bucket, in as little as two inches of water.
Two inches of water or six feet of bubbles!
Intentional Harm
People are more likely to be killed by people they know than by a stranger, and it will probably be in the victim’s home.
As of 2017, 12.3% of homicide victims were killed by family members, 28.0% were killed by someone they knew other than family, and only 9.7% were killed by strangers. In 50% of cases, the relationship between the victim and the offender were unknown. Chances are, at least some of those were family or acquaintance homicides.
Approximately 39% of victims were murdered during arguments or as a result of romantic triangles. Another 24.7% of murders were committed in conjunction with another crime such as rape, robbery, burglary, etc.
More than 72% of the known weapon homicides involved firearms, primarily handguns.
Violence against women—Domestic violence is the #1 cause of injury to women, more than all the rapes, muggings, and car accidents in a given year.
One out of every four women in the U.S. will be injured by a husband/lover during her lifetime.
64% of women killed each year are murdered by family or lovers.
Violence against children—Calls to Child Protective Services received 3-4 million reports of alleged abuse in 2011: 79% neglect, 18% physical abuse, 9% sexual abuse.
Babies under the age of one were assaulted most often. Of child victims in 2011, 82% were younger than four.
Children in violent homes have sleeping, eating, and attention problems.
Abused children are more withdrawn, anxious, and depressed than non-abused children.
Pictured above: not a neglected or abused child. Still, railings are a good thing.
Bottom Line For Writers: whether accidental or intentional, injury and death are fertile ground for tension, emotion, and upping the stakes.
Today is What You Think Upon Grows Day. It’s a day to remind oneself and others of the power of positive thinking. Studies have shown that there is a major difference in the lives and health of optimists and pessimists.
Positive thinking doesn’t mean that you keep your head in the sand and ignore life’s less pleasant situations. Positive thinking just means that you approach unpleasantness in a more positive and productive way. You think the best is going to happen, not the worst.
Positive thinking like this does lead to health benefits, such as:
Increased life span
Lower rates of depression
Lower levels of distress
Greater resistance to the common cold
Better psychological and physical well-being
Better cardiovascular health and reduced risk of death from cardiovascular disease
Better coping skills during hardships and times of stress
If you consider yourself a negative thinker, it’s a good idea to identify those negative thoughts and begin to reprocess them as positive. For instance, if you think to yourself, “There’s no way this will work,” you can rephrase the thought to say, “I can try to make this work.”
Remember, these thoughts and actions do not go away overnight. It takes time and practice to become a positive thinker. Why not start on What You Think Upon Grows Day? It might be the perfect start to a new, healthier lifestyle.